
A third of Shasta’s jail deaths in recent years have been ruled suicides. A policy change could save lives
Two dozen people have died while incarcerated at the Shasta County Jail over the last six years. A review of postmortem investigations indicates more intensive monitoring of high-risk individuals could prevent deaths.

Editor’s Note: This story contains graphic details of suicide. If you or someone you know is in crisis, help is available. The National Suicide Prevention Lifeline is available by calling or texting 988. You can also chat online at 988lifeline.org or text HOME to 741741 to connect with a crisis counselor.
This is the first of a two part series on the death rate at the Shasta County Jail. This reporting was supported by the Center for Health Journalism’s 2026 California Health Equity Fellowship.
The Shasta County Jail has beds for 484 detainees. The fortress-like facility in downtown Redding towers above nearly everything around it. Typical of jail architecture, its brutalist build is heavy and modular, broken up by slit-like windows that reveal little of its interior.
For years, what happened behind those windows — the everyday lives of the incarcerated, along with details about their deaths — has been similarly shielded from public oversight.
Since 2020, 24 of the men and women who walked into the facility did not walk out, having experienced some kind of fatal health crisis while behind bars. The vast majority of those who died were still waiting for their day in court. Consistent with national trends, the most common cause of death in the jail over the last six years has been suicide.
Recent changes in state law have opened a narrow window into the jail’s inner workings in the wake of incarcerated deaths, providing access to investigative documents. In each one of these post-mortem examinations, there is a story to be exhumed, providing crucial details about the medical histories of decedents, how soon they died after being booked, how isolated their environment was, and in some cases, the level of anguish they were experiencing in the last days of their lives.
Analysis of those deaths reveals important consistencies, particularly among deaths by suicide.
Records show that the majority of those whose deaths were ruled suicides — eight out of nine — had documented histories of serious mental health disorders. All but one of the suicides occurred within a month of the individual being locked up, sometimes within just days or even hours of entering the jail. At least three occurred in isolation and five in the presence of a cellmate, although not every investigative report noted this information.
Jail staff reportedly followed the Shasta County Sheriff’s Office’s standards of care for those who died, which include welfare checks that occur once an hour for most individuals and twice every 30 minutes for those being closely monitored for psychiatric reasons or for substance withdrawal.
This level of observation does not seem to have been enough. Documents show that high-risk individuals — those who had been showing clear signs of a potential substance use withdrawal or suicidality, or both — consistently died in between those periods of monitoring. Four of the deaths occurred in the parts of the jail that are the most intensely monitored, during the mere minutes they were left unsupervised.
The data about these deaths indicate that lives could be saved by implementing closer monitoring of high-risk individuals including 24/7 observation of those in an acute crisis. Adding more frequent monitoring checks among the general population during the first few weeks of incarceration could further reduce risk of death.
Elected officials have acknowledged the jail’s high death rate. But as bodies piled up over the last six years, county staff have never conducted a public-facing review of the patterns behind those deaths.
Neither the Shasta County Board of Supervisors nor Shasta Sheriff Michael Johnson responded to requests for comment on the specifics of this story, including the patterns of deaths and the feasibility of monitoring .
The sheriff did not confirm or deny whether his staff have ever conducted an audit of the deaths, and if so, what their findings were. A review of every amended version of the sheriff’s jail policy manual spanning back to 2019 shows that monitoring policies have remained nearly unchanged.
In-custody deaths at the Shasta County Jail, 2020–present
The following data was pulled from a combination of sources: Shasta County’s mandatory in-custody death reporting, the available post-mortem investigation documents for those who died behind bars, and state-wide data from the California Department of Justice on in-custody deaths.
| Name | Age | Died | Days in | Cause | Cell type | Pretrial | SMI or NCD* | Known substance use | Cellmate | Suicidal |
|---|
*Serious mental illness or neurocognitive disorder
The designation of “unknown” refers to files that have not yet been released, or information that could not be obtained due to redaction or absence from the documents. All of the information in this graphic comes from documents internally produced by law enforcement. At least one family, that of Cody Jones, does not trust the coroner’s suicide ruling and suspects correctional officers may have been involved. The sheriff did not respond for comment. Graphic created by Madison Holcomb and Nevin Kallepalli.
The case of Juan Moreno
In the early hours of Jan. 24, 2025, Deputy Coroner Josh Dorstand pulled into the Shasta County Jail parking lot.
“It was dark outside, and the weather was cold and fair,” he later wrote in an investigative report. He approached cell #4. The door was ajar. He observed little out of the ordinary in the cell itself, but on the ground in front of him was the body of a young man.
He was “lying supine,” Dorstand wrote, the majority of his body shrouded in white fabric.
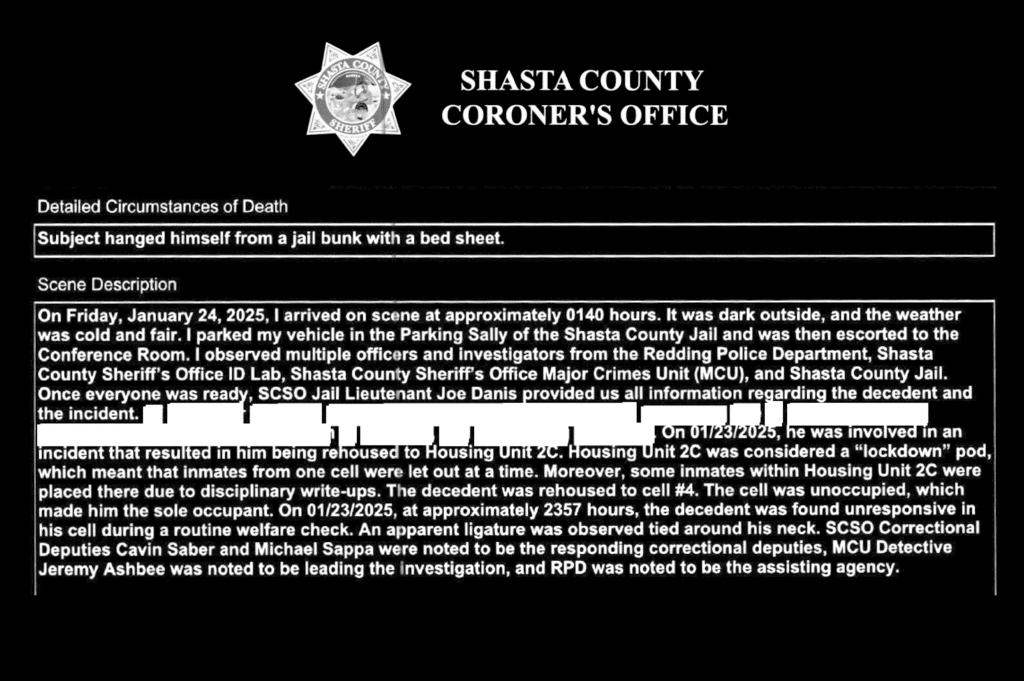
Juan Moreno was 27 years old when he died by hanging, according to his autopsy report, having apparently fashioned a noose from a bedsheet.
Exactly 11 months later on Christmas Eve, Moreno’s mother, Ana Arroyo Rodriguez, filed a lawsuit at the Shasta County Superior Court, just down the street from where her son had been discovered unresponsive.
The lawsuit accused the county of alleged negligence and medical malpractice, along with violations of the Ralph Act and Bane Act — both of which relate to civil rights based on perceived race, disability, gender, religion, sexual orientation and other immutable qualities.
“The death of Juan Moreno was completely unreasonable because [he] should have been monitored and receiving medical care while in County of Shasta custody,” the civil complaint said.
The document details Moreno’s life before he was escorted into the jail in shackles, describing how he came of age while battling serious mental illness. According to the complaint, Moreno was in elementary school when he first started hearing voices. His first incarceration was at the age of 12. Along with his mental health challenges, Moreno later took to substance use. He fled from rehabilitation and psychiatric facilities over the next 15 years of his life, according to legal filings.
Moreno’s medical records were obtained by the sheriff’s office only after his death, as part of his post-mortem investigation. Those records indicated he had been involuntarily hospitalized just 11 days before his arrest while in the throes of a psychiatric crisis that involved thoughts of homicide.
He was incarcerated after allegedly breaking into his father’s house and stealing his truck before evading police on foot. Police records also outline an incident of fire-starting at his mother’s house that was driven, the report said, by hearing voices coming from a large pile of debris.
Christian Contreras is an attorney based in Southern California who’s taken on Moreno’s case, which is scheduled for trial in September.
“I get it; a lot of these cases may not be intentional,” Contreras said by phone, referring to deaths like his client’s. “We’re not saying that Shasta County is murdering people — but at the same time, they have huge responsibilities.”
As Contreras pointed out, prisoners have a unique constitutionally protected right to health care and are the only people in the United States who are guaranteed such care. The county has an obligation to protect those in custody from physical harm, he added, which includes self-harm.
Protocols are already in place in Shasta’s jail for how to respond to individuals who pose a threat to themselves or others. Jail staff are required to undergo specialized training, report suicidal ideation or attempts, and maintain “open lines of communication” with one another if someone has shown signs of suicidal intent. The jail also utilizes safety cells, which can be used to house people considered high risk because they pose a threat to themselves or others.
Safety cell legislation prohibits placement in these rooms as a form of punishment. California building code outlines their basic requirements: Safety cells must be at least 4.5 square feet of floor space with a shutter for food delivery and no internal control of lighting. For those placed in safety cells during a psychiatric crisis, the only view to the outside is a small window on the door.
In Shasta, once placed in a safety cell, the individual is required to be visually observed at least twice every 30 minutes at irregular intervals. Within 12 hours of placement in a safety cell, medical staff are required to use a medical screening to determine whether the individual should be retained in the safety cell, released into general jail housing or referred for advanced treatment at a hospital, something the county would have to pay for.
Unlike Shasta, which has no policy manual section focused on “suicide watch,” the jails in both Butte and Tehama Counties outline standards for this practice, during which actively suicidal individuals are continuously monitored by a correctional officer, with the option of added video monitoring.
Similarly, Sacramento County jails — each with a daily population of around 1,500 — utilize “continuous observation” of those deemed suicidal until they’re able to see a mental health professional. That’s similar to both the California state prison system and the Federal Bureau of Prisons, which require constant visual monitoring of someone deemed high risk.
Contreras said it’s important to remember that anyone can end up in jail, and such people are, by definition, innocent until proven guilty.
“Even if someone did something wrong, a human being is dying unnecessarily,” he said, emphasizing the importance of care for the incarcerated. “His mother misses him deeply. … She wants justice, she wants accountability, she wants reform.”
Spanning back six years, Moreno was just one of nine people at the Shasta County Jail whose autopsy reports show that they took their own lives. Eleven more died from overdoses, withdrawals and other medical emergencies compounded by COVID-19 or chronic health conditions like Alzheimer’s, heart disease, diabetes and HIV. Two of the deaths at the jail are still under investigation.
The jail as a treatment center
In the 1970s, J.W. Gamble — an incarcerated man in Texas who was injured when a bale of cotton fell on his back during a prison work assignment — sued the Texas Department of Corrections. His lawsuit, which was eventually heard in the U.S. Supreme Court, alleged he was subjected to “cruel and unusual treatment” due to the prison’s allegedly subpar standard of health care. While the court ruled against Gamble, the case established that a prison’s “deliberate indifference” can constitute cruel and unusual punishment, a violation of the Eighth Amendment.
The landmark ruling also made clear that jails and prisons are, in part, health care facilities.
The Gamble case is a pivotal precedent for Moreno’s, when active mental illness leads to alleged criminal conduct, landing someone in a jail cell rather than an emergency department.
In California, residential health care facilities like hospitals and in-patient psychiatric facilities routinely deploy 24/7 “constant visual observation” for suicidal patients. By contrast, Shasta’s jail policy permits at-risk individuals in safety cells to be checked on only intermittently, despite the fact that isolation is known to increase suicide risk.
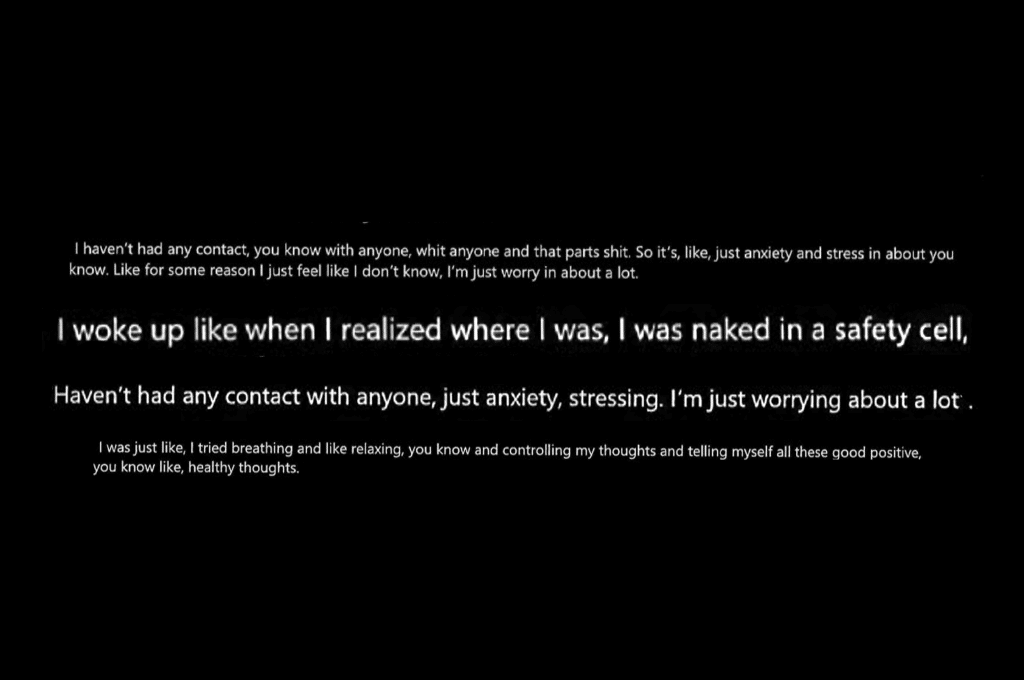
While Moreno made documented suicidal statements during his first month in jail, he was never placed in a safety cell, according to investigative documents, which don’t indicate why this step wasn’t taken. He was initially housed with a cellmate then moved alone to a different cell after allegedly fighting. In that cell he received hourly visual monitoring, the standard for housing cells that aren’t suicide or sobering specific. Less than eight hours after that placement, he took his own life.
Dr. Amy Barnhorst, a psychiatry professor at the University of California, Davis, has experience working with jail populations. She recommends 24/7 monitoring for incarcerated patients in an acute psychiatric crisis who pose a risk to themselves — whether it be by video or with in-person monitoring.
That’s important in part, she said, because the extent to which her incarcerated patients were suffering was often hard to determine.
Medical intakes are routinely used in jails, including Shasta’s, to screen for suicide risk. But it’s a process limited to the individual’s ability to accurately self-report, as jails don’t have access to medical records. Making matters worse, many of those entering incarceration are arriving after traumatic arrests or amid psychiatric crises or active substance use, limiting their ability to share accurate insights about their state of mind.
“It’s really, really hard to get straight information out of somebody who is high or in crisis, or both,” Dr. Barnhorst explained. “They’re often very paranoid, for good reason.”
What’s more, the jail’s environment itself can be a significant trigger for new onset of suicidal thoughts.
“The amount of patience and waiting you have to do, with no progress and no information… I think it exacerbates the idea that I have no control to get myself out of this situation,” Barnhorst said. She was referring to individuals in pretrial detention, who often do not have regular access to their public defender or frequent contact with the outside world.
Barnhorst also expressed the need to find “more humane” ways of keeping people safe, noting that safety cells can feel anything but.
“They increase everything that makes people suicidal,” Barnhorst explained. “They’re cold, they’re uncomfortable. It’s humiliating, and they’re really undignified.”
Even without mental health or substance use complexities, jail environments present major obstacles to tending to patients, said Geneica Williams, a Wellpath nurse and union member at the Santa Rita Jail in the Bay Area. The biggest difference between a jail and a hospital, she said, is that incarcerated patients are not there by choice.
Williams said correctional care often requires nurses to go beyond what is technically required of them to slowly break down the psychological barrier between nurse and incarcerated patient in attempts to improve care. During conversations with patients, Williams said she asks if they’re jittery or sad, for example, trying to draw out more of their emotional state alongside their physical one.
“It’s all about the dialogue,” Williams added, noting that making time for such dialogue is challenging because nurses can be tasked with overseeing the care of numerous patients.
As a union member, Williams said she has consistently advocated for increased staffing to address the needs of complex patient populations in jail. In addition to a lack of medical records and the exacerbating conditions of incarceration, she explained, her patients are often particularly vulnerable to medical ailments due to their life circumstances before, during and after incarceration.
“They need care the most,” she said of the vulnerable individuals she serves. “Just because you’re homeless or just because you committed a crime does not mean that you’re not a person.”
Identifying windows of risk
“The important thing is to look at the common denominators.”
Those words are from Marc Bullaro, an adjunct professor at the John Jay College of Criminal Justice in New York and former assistant deputy warden at Rikers Island. Broadly speaking, he said, most suicides in carceral facilities occur within a short period of initial booking and in isolated cells, something that should inform each jail’s strategy.
Bullaro worked at Rikers, which can hold several thousands of incarcerated individuals, for 29 years. In recent years, the infamous jail in New York City has come under immense scrutiny due to the appalling conditions reported from the inside; 2022 was its deadliest year with 19 deaths. While high, that death rate, when assessed as a percentage of population, is still well below Shasta’s rate in the last six years.
Bullaro said he was involved in the post-mortem investigation process of about 50 jail deaths attributed to suicide. With his years of expertise as a veteran correctional officer, he has written about how he thinks New York’s jail system should be reformed and weighed on correctional procedures he believes would prevent people from taking their own lives.
There are standard policies that Bullaro said can mitigate risk, such as housing people in an area with a higher officer-to-inmate ratio in their first two weeks of incarceration, which increases oversight during one of the most hazardous periods for fatalities. He cited 1:1 suicide watch as an effective means of prevention, dormitory-style housing to avoiding isolating one or two cellmates as much as possible, along with peer-assisted suicide prevention programs — in which incarcerated people themselves are trained to spot and report signs of suicidality among the jail population.
But he acknowledged that the policy changes he recommends are always limited by a jail’s facility design, jail population turnover and manpower.
“The question becomes, ‘Is that practical? Is that realistic?’” Bullaro asked.
The Shasta Sheriff has expressed concern about the architecture of the county’s jail. He’s noted issues with overcrowding and indicated that the design of the aging facility also affects operations, including the morale of correctional staff. He’s discussed eventually building a new jail on the outskirts of Redding’s city limits, which if realized, would expand the jail’s blueprint significantly and could make room for more modern, and safer, facility design.
Despite such facility and staffing limitations, Bullaro is focused on what changes could be made in any given situation. Asked to what degree suicides in a jail are inevitable, he answered resolutely.
“I won’t agree — I can’t agree — that it’s just part of the job. Because there are a lot of things that can be done to prevent suicides.”

Tentative changes in care
While medical protocols play a role in how effectively suicides are prevented, the granular details of Shasta’s last contracted medical provider’s approach to suicide prevention remains largely unknown.
Shasta Scout was unable to obtain the policy manual of Wellpath, the private company that was contracted to provide medical services at the jail over recent years. In response to a records request, the sheriff’s office said it could not access the policy manual, despite the fact that the county was required by contract to approve that manual each year.
The county cut its ties with Wellpath this year, signing with the nonprofit MEDIKO instead in a contract that began on June 1. Johnson, who enthusiastically pushed for the new — and much more expensive — medical contract, said it would improve care, reduce legal risks and save money in the long run. Wrongful death lawsuits aren’t cheap, the sheriff reminded supervisors, as one made a snide remark about the bereaved “sue-happy” families that are “first in line” to file a lawsuit against the county after a jail death.
Dr. Kaveh Ofogh is MEDIKO’s CEO, a Virginia-based correctional health care company founded by Ofogh after he worked as a physician in an emergency department. He has stated to Shasta Scout that his company is “medically not financially driven,” nor is it owned by a massive private equity firm like Wellpath. During a recent interview, he said he planned to implement 24/7 monitoring for people designated to be at high risk and medically assess those in psychiatric crisis at least daily.
On April 7, Ofogh paid a visit to Shasta County. He attended that week’s supervisor meeting and was warmly introduced to the public by the sheriff himself before he addressed the county board. Ofogh spoke during the public comment period of the meeting, using his three allotted minutes of speaking time to emphasize that incarcerated individuals are just as entitled as anyone else to quality health care. He referred to them as “my patients.”
“They have someone outside who loves them,” Ofogh reflected. “They have a father, their mother, their brothers, their sisters, their children, and our job is to make sure we deliver proactive, compassionate—”
Ofogh was abruptly cut off by the three-minute timer that limits how long each member of the public can speak. Unlike other high-profile public presenters who have appeared at the forum to discuss relevant topics to the county recently, he was not allotted extra time to speak. Nor was he asked a single follow-up question.
Do you have a correction to share? Email us: editor@shastascout.org.
Related Articles

Inside the protests dividing the Redding Senior Center
Members of the senior center are calling for regular meetings and greater transparency after proposed bylaw changes that would eliminate statutory voting membership. Center leadership says the protesters represent only a small share of members.

‘I don’t like to limit me’: How North State Senator Megan Dahle continues to use her voice after a life-changing stroke
Megan Dahle, a California senator representing parts of northern California, is living with speech difficulties after having suffered a stroke in late 2023. Her principles, and style of representation, she said, haven’t changed.

Shasta’s Health and Human Services Agency warns against scam phone calls
Criminals have been falsifying their caller ID and impersonating county employees to deceive residents, Shasta’s HHSA warned today.
Comments (0)
There are no comments on this article.